
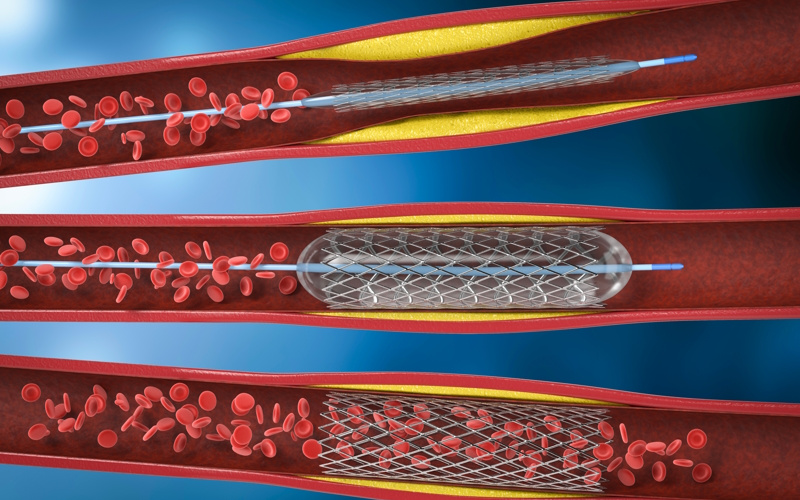
Cardiac catheterization is used to investigate the structure and function of the heart. Coronary Angiogram is used to investigate for any narrowing of the coronary arteries (arteries that supply blood to heart muscle). When indicated, percutaneous coronary intervention (PCI) can be performed at the same setting of cardiac catheterization and coronary angiogram.
Atrial fibrillation is a common heart rhythm disorder in which patients typically experience an irregular, extremely fast heart rhythm. Here there are the three types:
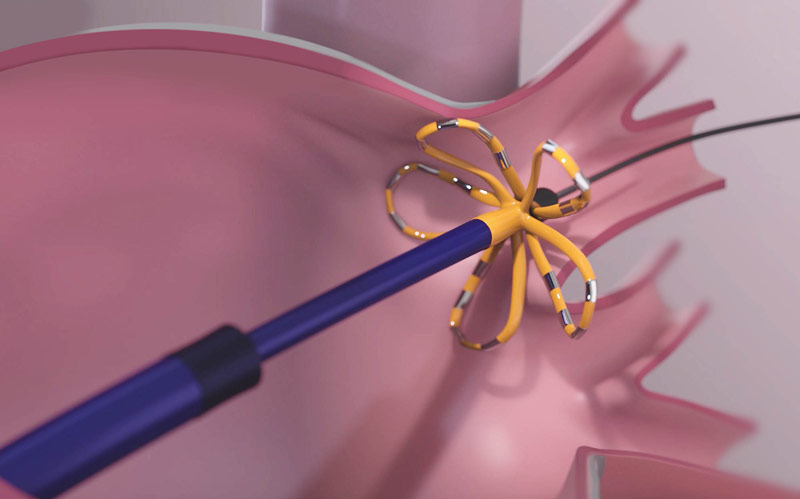
Atrial fibrillation is a common heart rhythm disorder in which patients typically experience an irregular, extremely fast heart rhythm. Here there are the three types:

Heart rhythm is mainly controlled by the conduction system of the heart. Any abnormality in the conduction system may result in abnormal heart rhythm (arrhythmia).
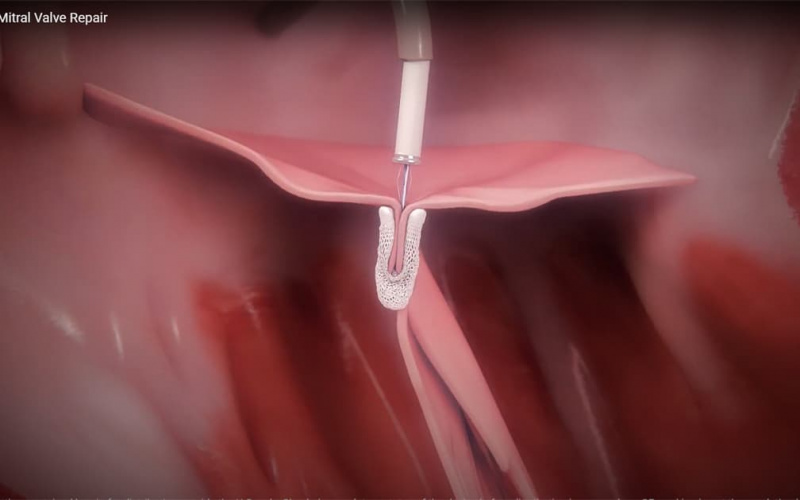
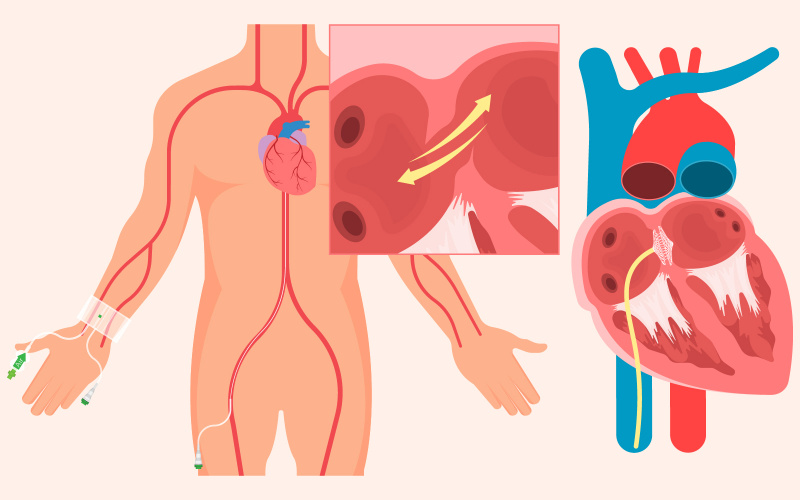
Mitral regurgitation (or “MR”) is a condition affecting one of the valves in your heart, the mitral valve. The valves in your heart control the flow of blood through the four chambers of your heart. Each heart valve is made up of thin, but strong flaps of tissue. As blood flows through the four chambers of the heart, the valves open and close to ensure that blood flows in the right direction.
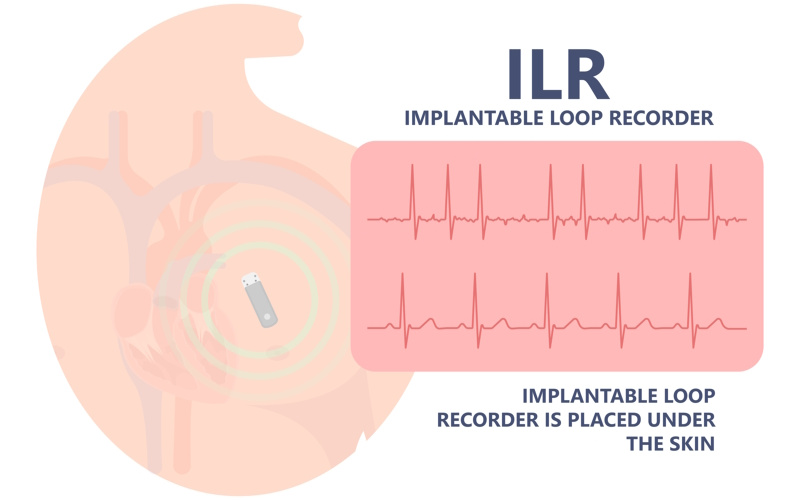
Patients may have unexplained recurrent symptoms of dizziness, palpitation or loss of consciousness. There are many causes, such as arrhythmias (abnormal heart rhythm). Sometimes, a definitive diagnosis cannot be made after conventional investigations.
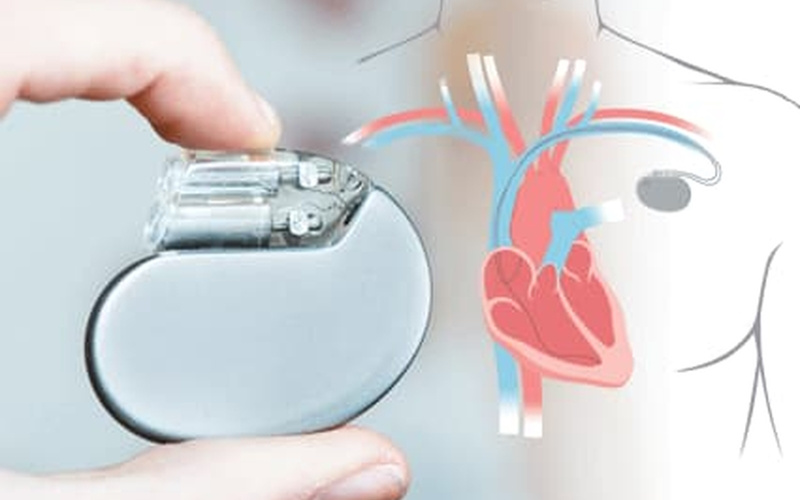
Heart rhythm is mainly controlled by the conduction system of the heart. Any abnormality in the conduction system may result in abnormal heart rhythm (arrhythmia). Arrhythmias with slow heart rate cause dizziness, syncope, heart failure or occasionally cardiac death.

Heart failure patients have symptoms of shortness of breath and body swelling caused by decreased pumping of blood from the heart. Initial management includes treating underlying cause, adopting a healthy lifestyle and taking medications.

Heart rhythm is mainly controlled by the conduction system of the heart. Any abnormality in the conduction system may result in abnormal heart rhythm (arrhythmia). Life-threatening arrhythmias such as ventricular tachycardia (VT) and ventricular fibrillation (VF) cause not only palpitations, dizziness and syncope but also sudden death.
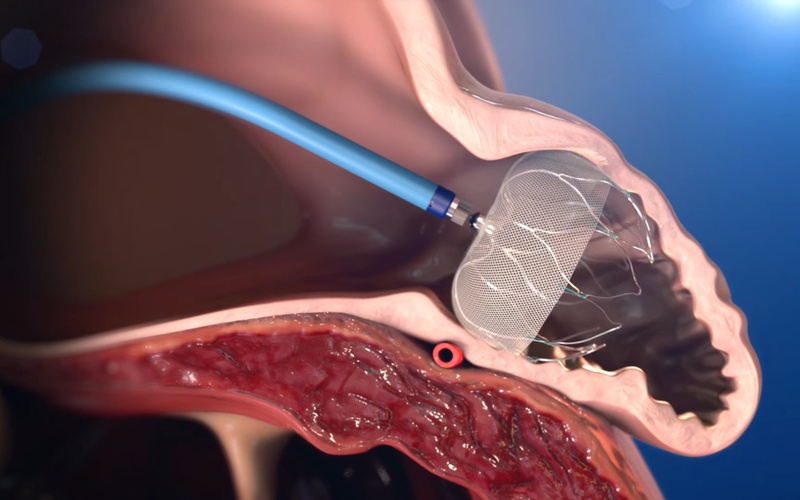
Atrial Septal Defect (ASD) is a common congenital heart disease. A hole in the septum between the left and right atria causes abnormal blood shunting, which increases the burden on the heart.
Additionally, the Patent Foramen Ovale (PFO) is located between the left and right atria. In most people, it closes naturally after birth. If it remains open, it is called a PFO. While adults with this condition can lead normal lives, it can increase the risk of blood clots.
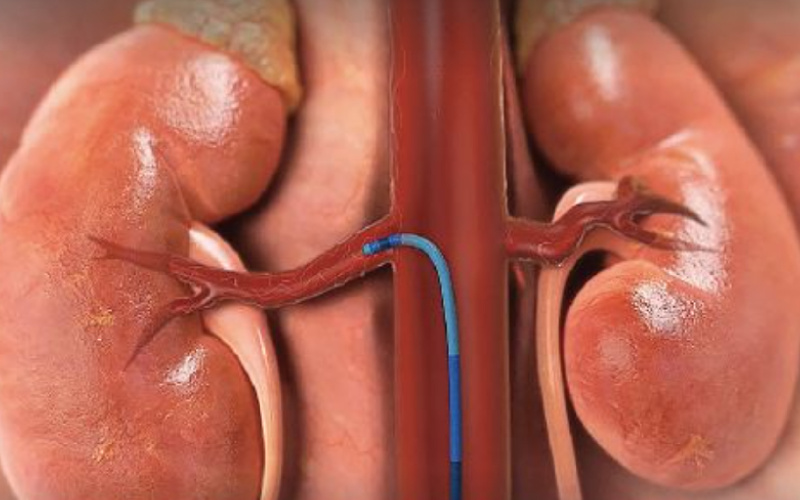
透過腎臟交感神經消融術,將過度活躍的交感神經切斷,減低荷爾蒙腎素的分必量,從而降低血壓水平,保障病人心臟,腎臟及血管健康。